Chest wall deformities are often referred to as ‘Pectus’ and are relatively common conditions. This is when the chest wall appears irregularly shaped. Most are often noticed in childhood around the ages of 3-5, but often they can present in early adolescence. They often get worse during the child’s growth spurt, around the time of puberty and then stabilise in appearance once they have reached adulthood.
The two most common forms of Pectus deformity are Pectus excavatum and pectus carinatum. Pectus excavatum (which is sometimes called ‘Sunken Chest’) is when there is a cup like deformity usually located in the lower part of the chest. Pectus Carinatum (which is sometimes referred to as ‘Pigeon Chest’) is when there is a protrusion of the chest wall.
WHAT CAUSES PECTUS?
The exact causes of pectus deformities are still unclear. Some researchers believe that it is a congenital disorder as it tends to run in families (1 in 4 individuals have close family members with a similar problem). No specific gene defect has yet been found but it is likely that there is a significant genetic element. It is believed to be caused by an abnormal growth of the cartilage that connects the ribs to the sternum. Most pectus deformities are found in isolation, but they are often associated with a number of other musculoskeletal problems. These include scoliosis (curvature of the spine) and connective tissue disorders (such as Marfan’s, Ehlers Danlos syndrome).
Pectus excavatum
Pectus excavatum (which is sometimes called ‘Sunken Chest’) is when there is a cup like deformity usually located in the lower part of the chest. It is the most common pectus deformity and is likely caused by abnormal growth of the cartilage that connects the ribs to the sternum. It can sometime present in children at the ages of 3-5, but becomes much more apparent when they grow older and during puberty with their growth spurt.
SYMPTOMS
Pain – One of the most common symptoms, especially during the growth spurt. It can sometimes also affect the back and is often intermittent in nature. It is typically worse during heavy exercise.
Feeling out of breath – Sometimes patients can feel a sense of breathlessness when doing exercises and is often noticed during sports activities in school.
Palpitations – in some cases patients are more aware of their heartbeat. This can happen in severe pectus deformities when the heart is displaced.
Syncope – In some rare cases, patient have described syncope (feeling faint) typically when excersing.Again this is thought to be due to the distortion effect of the heart when it is displaced.
Psychological – perhaps the most disabling symptom for a lot of the patients. It can have a profound effect on the patients confidence , mood and self-esteem.
Not all of the above symptoms are present in all patients. Pain in the chest is quite variable and some patients don’t have any chest pain at all. The psychological impact on pectus can be very disabling and is often the one that patients are most concerned about. It often leads to a change in behaviour such as withdrawing from sports activities in school (i.e. swimming) and not being able to enjoy holidays.
DIAGNOSIS
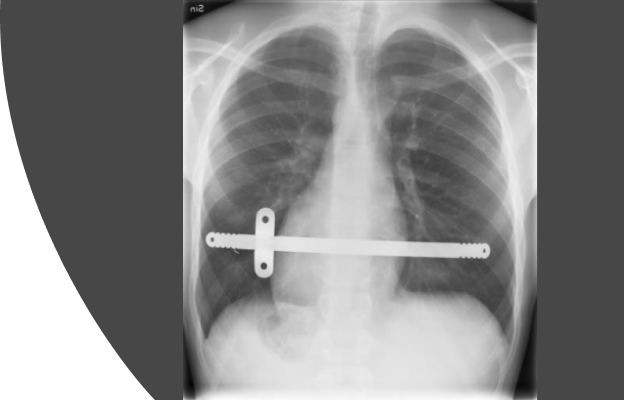
Diagnosing pectus excavatum is usually relatively straightforward when physically examined by a doctor who is familiar with pectus deformities. No specific blood tests or imaging is required to diagnose pectus. However, imaging of the chest is very helpful in determining how severe the pectus is as well looking at the heart and the spine to see if they are affected.
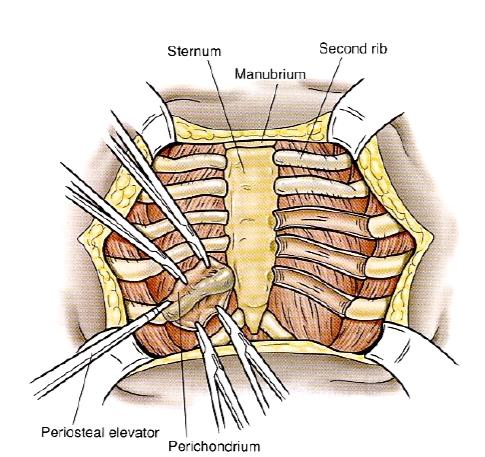
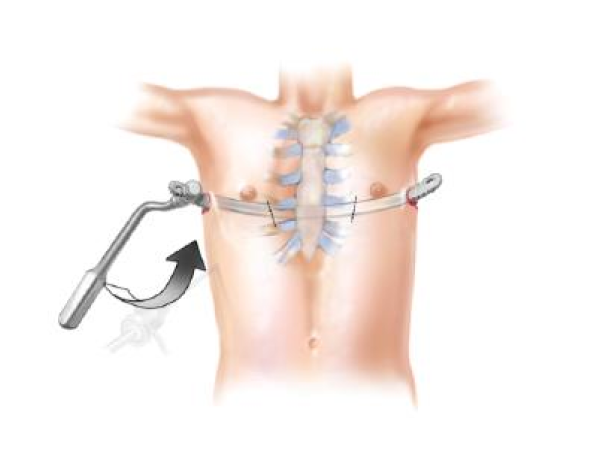
Usually the first scan we recommend is a chest CT scan for pectus excavatum. This usally tells us exactly how deep the sternum is pushed back in relation to other organis in the chest. It will also allow us to produce a 3D image of the chest where we can see the outline of the deformity and assess what treatment options may be feasible. in particular, this will help us decided what type of surgical repair might be necessary (i.e. NUSS bar vs open procedure). Other scans, particularly in children such as MRI which avoids radiation can give us similar information.
We often get other investigations to look specifically at other organs in the chest. For example an echocardiogram (which looks at the heart) and well as lung function tests to see how the lung is working.
Pectus Carinatum
Pectus Carinatum (which is sometimes referred to as ‘Pigeon Chest’) is when there is a protrusion of the chest wall and is the second most common chest wall deformity. It usually comes on slightly later than pectus excavatum and typically tends to get worse during the growth spurt and puberty.
SYMPTOMS
The symptoms are very similar to pectus excavatum with patients describing chest pain and breathlessness when doing heavy exrcises. Many patients often don’t have any symptoms at all. Similar to pectus excavatum, the effect on self-confidence and body image is what usually brings them to see a doctor and can be devastating for patient at a crucial time of their lives.
DIAGNOSIS
Diagnosing pectus excavatum is usually relatively straightforward when physically examined by a doctor who is familiar with pectus deformities. No specific blood tests or imaging is required to diagnose pectus carinatum.
We do sometimes recommend a CT scan, especially for more complex cases of pectus carinatum to outline the shape of the chest wall. We often don’t need an echocardiogram or lung function as there usually is no compression to the organs inside the chest.
Most of the time we can use optical scanners to look at the chest wall and guide treatment using braces and avoids radiation.
Rib Flare
As we have mentioned earlier pectus deformities are often associated with other conditions. One of the most common associated pectus abnormalities is ‘Rib flaring’. It typically affects the lower ribs where they appear as if they are sticking out. It can also occur in isolation without any pectus deformity.
Rib flaring can happen in both pectus excavatum and carinatum and it can affect either one side or both sides. Indeed, some patients complain that the rib flaring is their most significant deformity masking the underlying pectus.
Treatment for rib flare is often using a brace. In patients with a pectus deformity, treatment of the underlying pectus can sometimes improve or worsen the rib flaring. This can be treated at a later stage.