We have been using braces for pectus Carinatum since 1996 and have had used them in 1000’s of patients worldwide. Bracing is now considered first line treatment for pectus carinatum across the world and has also been approved by the American Paediatric Surgical Association.
The role of bracing in pectus excavatum is less established. We run a clinic along with a bracing technician who is an expert in the field. Measurements are taken at our clinic using 3D light scanners and a custom-made brace for each patient is made.
A detailed individualised plan for each patient is made once the braces have arrived from the USA with step-by-step guide to bring the chest back to a normal shape.
Vacuum Bell Therapy
The vacuum bell device has been used since 2005 and has gained popularity since then. It offers a unique non-surgical treatment method for the treatment of pectus excavatum. Essentially it is a vacuum device which is placed over the sunken part of the chest . Although not used regularly for the sole treatment of pectus excavatum, it is now being used in young patients who have more flexible chest walls as a long term treatment solution.
We will assess the best method of treatment after our initial consultation and whether this may be a feasible treatment method. The device has to be worn several hours a day for up to 12 months in patients who have a pliable chest wall (which we will be able to assess at the consultation).
SURGERY
Surgical correction of pectus deformities is important to consider when deciding on the best treatment option. Surgery can be used in both pectus excavatum and carinatum, although the first line recommended treatment for carinatum is leaning heavily towards bracing.
Some non surgical methods do exist for pectus excavatum (such as Vacuum Bell Therapy) although they are not suitable for all patients and all deformities. Surgery for pectus excavatum is usually thte most common treatment and is usually between three choices:
Implants
NUSS Insertion
Ravitch Procedure
The choice of operation will depend on a number of factors which we will discuss in detail with you at the clinic. It is important to go through each type of operation, their risks involved as well as their long-term cosmetic and functional outcomes.
The decision to have surgery is largely dependent on the severity of the pectus deformity and any associated functional/psychological issues. We will assess you with various investigations as required and go through in detail or recommendations and the rationale behind them.
PECTUS IMPLANTS
This is the least invasive and with the lowest risk of the three surgical options to treat pectus excavatum. It involves placing an implant under the soft tissue to hide the deformity. It must be remembered that it doesn’t correct the actual deformity and if there are underlying functional issues such as breathing difficulties or pain, this may not treat those.
The choice of implant over the years has changed and improved significantly. Recently we have been able to source custom made implants that is specific to each patient and vastly improves the cosmetic results. We work together with Mr Simon Withey a leading Consultant Plastic surgeon who specialises in the chest wall reconstructive surgery.
NUSS PROCEDURE
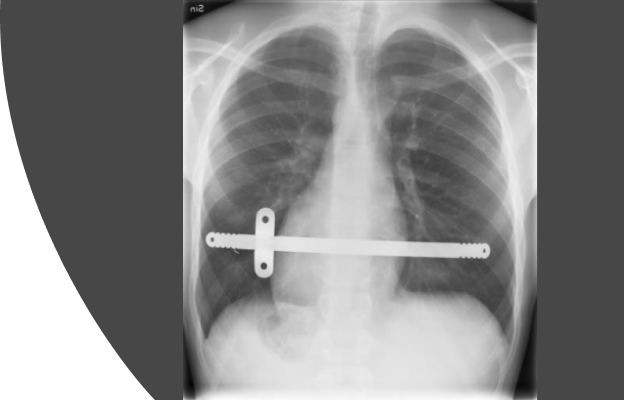
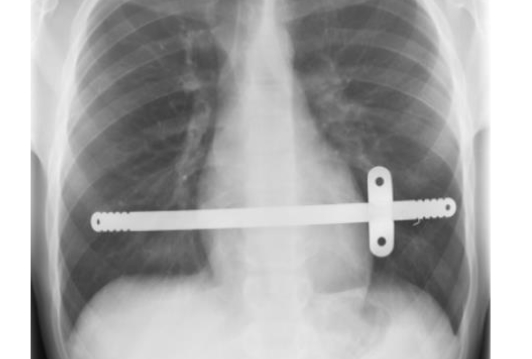
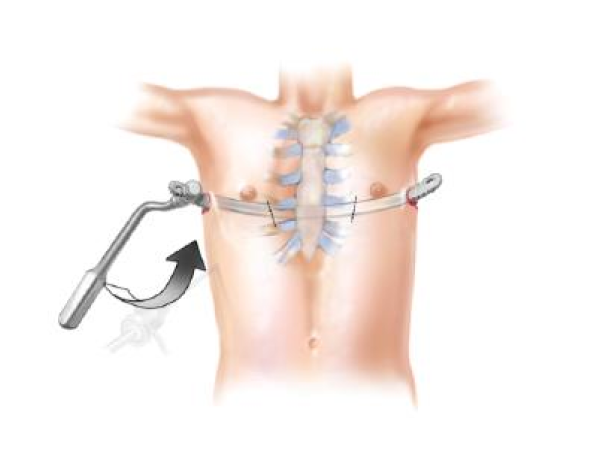
The NUSS procedure, first described by Dr Donald Nuss in 1987, has undergone several modifications to treat pectus excavatum. It is now essentially a minimally invasive technique that involves 1 or2 small incisions on the chest wall through which a metal bar (NUSS Bar) is inserted using keyhole technology to lift the sunken chest to a normal appearance.
It usually requires only 1 or 2 bars (rarely 3) which are then fixed in place. It provides almost immediate correction of the pectus deformity, with the bars remaining invisible on the outside. It takes between 1-2 hours to do the operation.
Hospital stay is around 2-3 days with the majority of the recovery focusing on pain on movement. Sometimes a drain may be required if there is a leak of air into the chest cavity during the operation. This usually settles within 24-36 hours.
Once discharged, patients can slowly return to normal activity with an emphasis on restricted heavy exercise for the first couple of weeks (such as heavy lifting or contact sports). The bar stays in for roughly 3 years. A follow-up appointment is made two weeks after the procedure and then at yearly intervals with a chest X-ray to ensure the bar hasn’t moved. The bar is then removed with another procedure which often takes approximately 30 mins and requires a 1-day hospital stay.
The NUSS procedure is a well-established surgical procedure for the treatment of pectus excavatum and we have performed hundreds of these over the last few decades with excellent outcomes.
Modified Ravitch Operation
The Ravitch procedure was first described in 1949 by Dr Mark Ravitch. It is significantly more complex than a NUSS procedure and involves a cut down the middle of the chest. Essentially it involves exposing all the cartilage that connects the ribs to the breastbone which are then excised as well as a cute through the breastbone itself. This frees up the chest wall so that the breast bone can be lifted up in the case of a pectus excavatum, or pushed back in for pectus carinatum. Often a bar, similar to the NUSS bar, is also used to hold the new position in place which is removed 1-2 years later.
For the majority of patients with pectus excavatum the Nuss procedure is often preferred and for pectus carinatum , bracing is preferred. However, the severity and complexity of the pectus deformity may necessitate this procedure. We will talk to you in details about all the options available and the benefits and cons of each one. Generally the Ravitch procedure is often performed in older patients (whereby the sternum is more rigid and less amenable to bracing or NUSS bars).
The operation takes around 2-3 hours to perform and most patients stay in for about 3-5 days. Recovery is generally longer than a NUSS procedure and can take up to 10 weeks before full recovery and a return to normal physical activities. Follow up is usually around 2 weeks after discharge with bar removal (if needed) around 1-2 years after.